
The consequences of infections involving the coronavirus SARS-CoV-2 are decreasing. This is because nearly everyone in the Netherlands has built up immunity to COVID-19 as a result of vaccination and/or previous infection, and because the current Omicron variants are less likely to cause serious illness. These insights have become apparent over time by connecting data from different sources, such as the National Sewage Surveillance, the National Intensive Care Foundation (NICE) and pathogen surveillance in the Netherlands.
Since the start of the pandemic in 2020, various SARS-CoV-2 variants have emerged in succession. Since 2022, most of the variants circulating in the Netherlands have been in the Omicron lineage. Compared to the Alpha and Delta variants, the Omicron variants are less likely to cause serious illness.
Virus particles in sewage in relation to hospital and ICU admissions
People who have a SARS-CoV-2 infection often excrete the virus in their stool, so virus particles can be detected in sewage. Since late 2020, RIVM has been measuring the number of SARS-CoV-2 virus particles in sewage to monitor how the virus is circulating in the Netherlands. This takes place in the context of the National Sewage Surveillance. Figure 1 shows the different waves of infection, displayed as hospital admissions (purple line), ICU admissions (green line), and virus particles in sewage (blue line, from 2021). The coloured areas in the background show which virus variants were involved and to what extent they were found in the Netherlands.
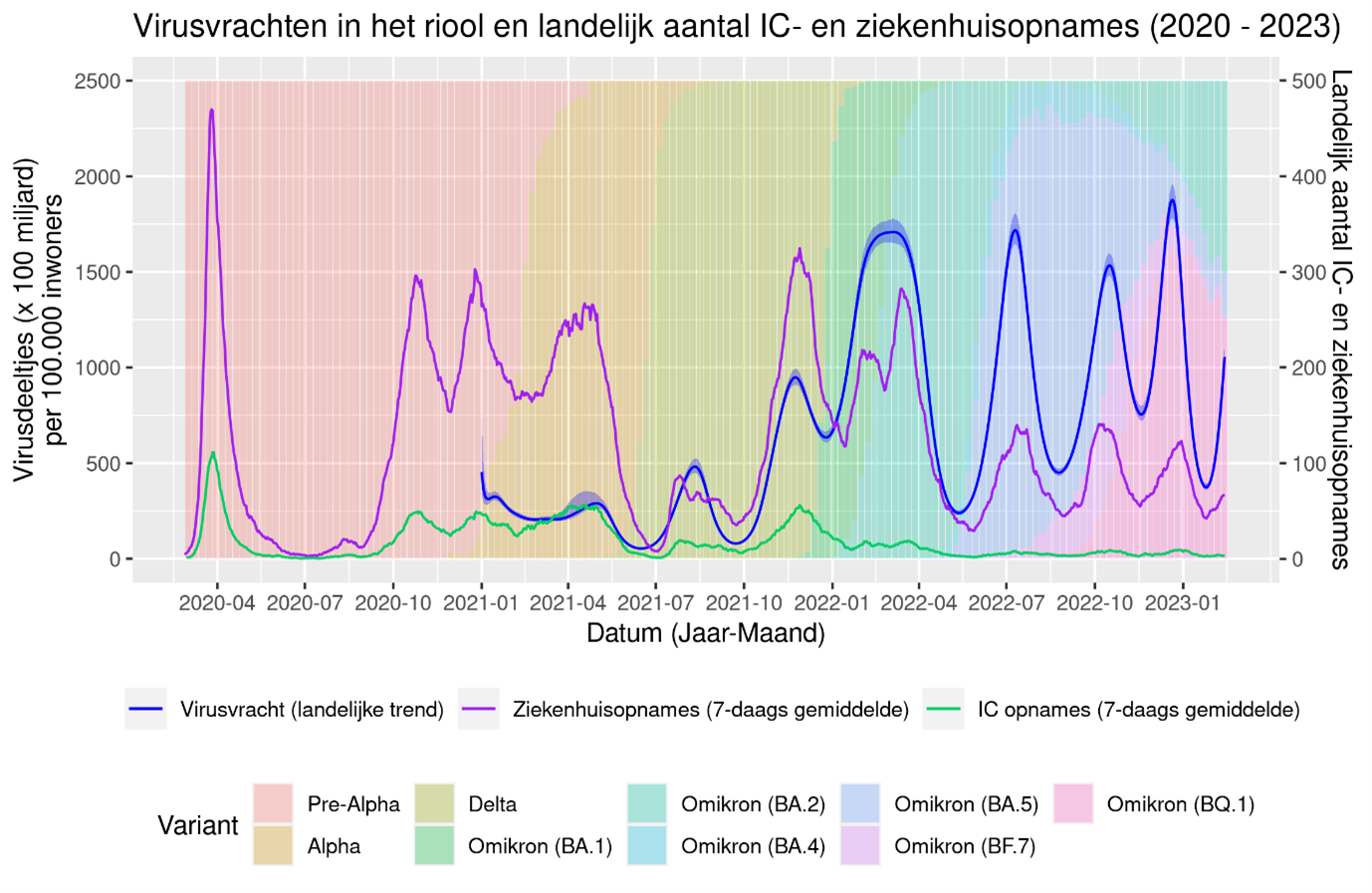
Figure 1: Average viral load (x100 billion) of SARS-CoV-2 in sewage surveillance (RIVM) and average number of hospital and ICU admissions with and due to COVID-19 (NICE) per day from 27 February 2020 to 13 February 2023. The coloured areas in the background show which variants were involved and to what extent they were found in pathogen surveillance in the Netherlands.
The number of hospital and ICU admissions offers an indication of the extent to which SARS-CoV-2 infections lead to severe illness due to COVID-19. The spikes in hospital admissions due to COVID-19 have diminished in height over time, even though the virus has been circulating more since the Omicron variants arrived in the Netherlands. The percentage of hospital admissions requiring ICU admission has also decreased over time, resulting in a relatively low number of ICU admissions since 2022.
Over time, there has been a change in how much the virus is circulating compared to the number of COVID-19 hospital admissions. This is displayed in Figure 2, which shows the number of hospital admissions (including direct ICU admissions) in relation to the number of virus particles in sewage. The downward trend indicates that a decrease in severe illness due to COVID-19 in relation to a certain level of virus circulation in the Netherlands. This does not mean that the virus is no longer dangerous to anyone. There are still groups of vulnerable people who have a higher risk of serious illness. During the period when the Alpha and Delta variants were circulating, hospital admissions were much higher in relation to levels of virus particles, compared to the Omicron variants that are now circulating in the Netherlands.
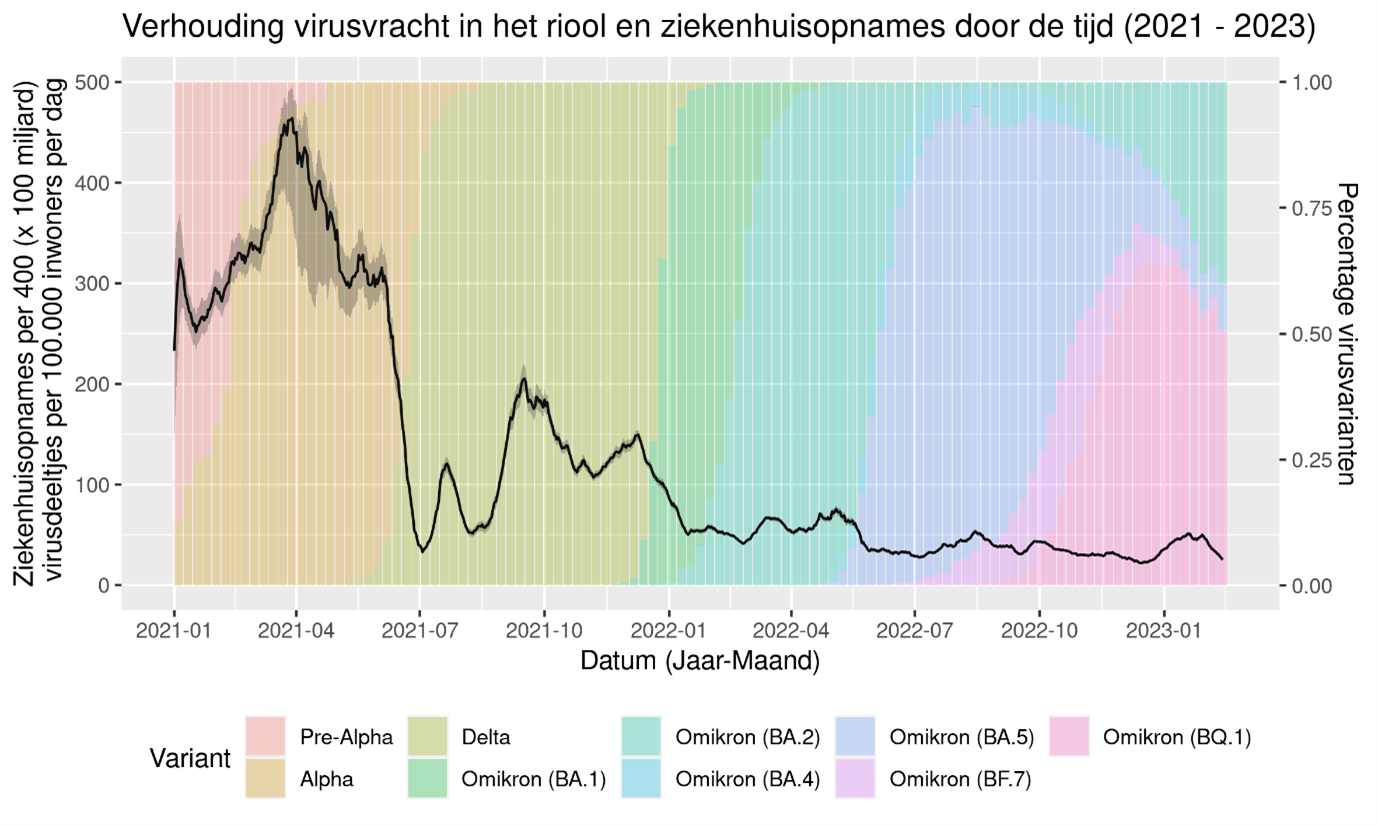
Figure 2. Average viral load in relation to number of hospital admissions (black) per day from 1 January 2021 to 13 February 2023. The coloured areas in the background show which variants were involved and to what extent they were found in pathogen surveillance in the Netherlands.
Continued monitoring of the virus
The Omicron variants of the coronavirus SARS-CoV-2 have now reached an endemic stage in the Netherlands. Effective surveillance remains important to maintain early detection of resurgences, new variants and changes in protection against severe illness due to COVID-19. RIVM will continue to monitor developments related to the virus based on various sources, including sewage surveillance, the Infection Radar survey, pathogen surveillance and hospital records.