
Vaccination coverage for vaccinations in the Dutch National Vaccination Program (NIP) decreased slightly by about half a percent for the third consecutive year. If this trend continues, the risk of future outbreak of measles increases. Compared internationally, vaccination coverage in the Netherlands is still high. This is shown by the Immunisation coverage and annual report National Immunisation Programme in the Netherlands 2016.
The slight-declining trend is visible for all NIP vaccinations for infants, toddlers and schoolchildren. This decreasing vaccination coverage increases the risk of future outbreaks, especially the highly contagious measles. A decreasing immunisation coverage increases the likelihood that diseases such as measles cause outbreaks in the future. A high degree of vaccination ensures that vulnerable (non-vaccinated) children are protected, this is called herd protection. The participation in HPV vaccine against cervical cancer has decreased for the first time, from 61 to 53 percent. Thus, there is an overall decline, which is visible in all Municipal Public Health regions.
International
A decreasing vaccination coverage increases the risk of a future measles outbreak, as currently in Italy, Germany and other European countries where vaccination coverage has also decreased. However, RIVM does not expect a measles outbreak in the Netherlands in the short term. In the Netherlands, still almost 95 percent of the population is vaccinated against measles.
In addition, the high risk group, namely the unvaccinated part of the orthodox Protestants, was exposed to the disease during the last measles outbreak in 2013-2014, which now reduces the spread risk. The World Health Organization (WHO) strives for a 95% vaccination rate for the first and second measles vaccination. This threshold is needed to achieve measles elimination. In the Netherlands this standard is no longer achieved
More knowledge, more information, more time
In order to gain more insight regarding the causes of the fall in vaccination coverage, further research will be conducted in the second half of 2017. This involves mapping possible causes in the social field. A committee of social scientists will advise on the way this issue can be addressed by the end of 2017. In addition, it will be investigated whether practical obstacles (accessibility) within the youth healthcare sector are a potential factor. RIVM is working on a renewed website on the National Vaccination Program to make vaccination information even more accessible to parents. RIVM will also make available an e-learning ‘Backgrounds of the NIP’ that will provide content-based knowledge for professionals. The e-learning will enable professionals to respond to many questions and concerns from parents and how to discuss them with them. As of January 1, 2018, more time will be available for this interaction.
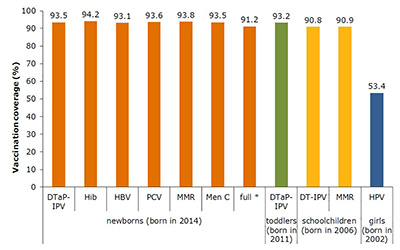
Vaccination coverage (%) per vaccine and birth cohort
Determined at 2 years of age (new-borns), 5 years of age (toddlers), 10 years of age (schoolchildren) and 14 years of age (adolescent girls).
Meaning abbreviations: D=diphtheria, T=tetanus, aP=pertussis, IPV=poliomyelitis, Hib=Haemohilus influenzae type b, HBV=hepatitis B, PCV=pneumococcal disease, M=mumps, M=measles, R=rubella, Men C=meningococcal C disease, HPV=human papillomavirus.
* full = all NIP vaccinations received according to schedule at 2 years of age.