Because most respiratory infections occur mainly in the winter, the data are presented for a respiratory season or a respiratory year. A respiratory year runs from week 40 of one year through week 39 of the following year. A respiratory season runs from week 40 of one year through week 20 of the following year. On this page, the data for 2024/2025 are limited to the respiratory season. More background information about the different surveillance sources can be found in the document 'Background and methods of the respiratory surveillance 2024/2025'.
About the influenza epidemic of 2024/2025
The influenza epidemic of the 2024/2025 respiratory season lasted from week 3 of 2025 through week 11 of 2025. The epidemic lasted nine weeks. This is based on data from all available surveillance sources (in Dutch) for influenza virus.
The number of people visiting the general practitioner (GP) with influenza-like illness (ILI) was above the threshold for increased activity (53 per 100,000 people) only during the first seven weeks of the influenza epidemic (week 3 to 9 of 2025). However, specimens from these patients and other surveillance sources showed that there was still increased circulation of influenza virus up to and including week 11. Influenza virus type A was most common this season. Influenza virus type B was found relatively little during the whole season, but the proportion of type B increased slightly at the end of the influenza season.
Mainly influenza virus type A
In the laboratory, testing is performed to determine the subtype or genetic lineage of the influenza viruses found. Of the specimens taken from people with an influenza-like illness who visited the GP, 20% had influenza virus subtype A(H3N2), 16% had subtype A(H1N1)pdm09, and 9% had type B of the Victoria lineage. Two of the A(H3N2) viruses were so-called reassortant viruses. In this case, it was a mix of the human A(H3N2) virus and A(H1N1)pdm09 virus. These viruses are likely related to an outbreak of respiratory infections at a school. Among Infectieradar participants with respiratory complaints (acute respiratory infection) who sent in a specimen to RIVM, 3% tested positive for influenza virus subtype A(H3N2), 3% for A(H1N1)pdm09, and 1% for type B of the Victoria lineage (see figure 2 on the syndromic surveillance page). Of the influenza specimens received by the National Influenza Center (Erasmus MC and RIVM) from diagnostic laboratories, a total of 1,479 viruses were subtyped. Of these, 36% were influenza virus type A(H1N1)pdm09, 29% were influenza virus type A(H3N2), and 35% were influenza virus type B of the Victoria lineage.
In all age groups, influenza virus A subtypes were found. B/Victoria was found most often in age groups under 50 years old. Worldwide, influenza virus type B of the Yamagata lineage has not been detected since the start of the COVID-19 pandemic in March 2020 (Caini, Meijer et al.). In October 2024, a small amount of genetic material of influenza virus type B of the Yamagata lineage was found in a patient with influenza-like illness who was sampled by a sentinel GP. Since the patient had not been vaccinated against influenza, vaccination had not yet started in the practice, and the patient had not had contact with people vaccinated with the live attenuated influenza vaccine, there is no indication of contamination of the specimen with the vaccine virus. Because of the low amount of virus in the specimen, the virus could not be cultured or sequenced. Therefore, infection with B/Yamagata virus could not be definitively proven. This finding has been reported and discussed with the WHO and ECDC. During the 2024/2025 respiratory season, the possible presence of B/Yamagata viruses in the Netherlands was closely monitored, but there were no further detections.
Illness from influenza
During the past respiratory season (2024/2025), the incidence of people with influenza-like illness caused by the influenza virus (symptomatic influenza) was estimated at 619 per 10,000 individuals. The estimated incidence is highest in the youngest age group (0-4 years). This symptomatic incidence of influenza is determined based on information about the number of people who visit the GP with influenza-like illness, the percentage of these people whose symptoms are actually caused by the influenza virus, and the likelihood that someone with influenza-like illness will visit the GP.
Reduced sensitivity to antiviral drugs
All the influenza viruses found through surveillance that have been sequenced are analysed for known genetic changes (mutations that lead to amino acid changes) that cause reduced sensitivity to antiviral drugs. The effects of these genetic changes on the phenotypic properties of the virus are also examined, together with wildtype influenza viruses for comparison. These tests assess the level of sensitivity of the viruses to the antivirals oseltamivir, zanamivir, and baloxavir marboxil. In the Netherlands, antivirals are infrequently used for treatment, only for people with a very high risk of becoming seriously ill from influenza. Among most of the tested A(H1N1)pdm09 and all A(H3N2) and B/Victoria viruses, no reduced sensitivity was found for oseltamivir, zanamivir, or baloxavir marboxil.
In the 2023/2024 season, a variant of A(H1N1)pdm09 was found with two amino acid changes, NA-I223V and NA-S247N, which caused a slight reduction inhibition by oseltamivir. This variant was not found in the 2024/2025 season. However, A(H1N1)pdm09 viruses with only the NA-S247N change were found. These had a higher half-maximal inhibition by oseltamivir, but not enough to be considered reduced inhibition. Three A(H1N1)pdm09 viruses had a NA-H275Y change, which causes a strong reduction in the inhibition by oseltamivir. In addition, one A(H3N2) virus was found with the NA-S331R change. This change was previously linked to reduced sensitivity to both oseltamivir and zanamivir. However, laboratory tests showed that this virus was still normal sensitive to both antivirals. One B/Victoria virus with the NA-M464T change showed a slight reduction in the inhibition by zanamivir. No viruses were found with amino acid changes that cause reduced sensitivity to baloxavir marboxil.
The NA-H275Y mutants can be considered resistant to oseltamivir and therefore cannot be treated with oseltamivir therapy. For the other mutants found, this is less clear, as there is little or no data on the treatment of patients infected with these mutant viruses. However, these mutants are less well inhibited by oseltamivir, which could make the treatment less effective.
Comparison of virus and vaccine
For the influenza A(H1N1)pdm09 viruses and influenza B viruses of the Victoria lineage, the vaccine composition for 2024/2025 matched well with the variants of these influenza viruses that circulated during the respiratory season in the Netherlands. Based on information available by the end of February 2025 for these viruses, no update of the vaccine for the 2025/2026 season was proposed by the WHO. Several influenza virus type A(H3N2) variants circulated worldwide at the same time, including the variant with a double amino acid change in the hemagglutinin protein (HA-N158K + K189R), which was at first mainly found in the Netherlands. This and some other A(H3N2) variants are less well recognized by the immune system of people who received the influenza vaccine in the autumn of 2024 or who have had influenza before. As a result, these people were probably less well protected against particularly the A(H3N2) (HA-N158K + K189R) variant. In week 50 of 2024, this variant was seen for the first time in the Netherlands. Its proportion increased each week to a maximum of 25% of A(H3N2) viruses that were sequenced. Because most A(H3N2) virus variants in circulation are well recognized by the A(H3N2) vaccine strain of the Southern Hemisphere vaccine for 2025, this vaccine strain has also been recommended for the 2025/2026 Northern Hemisphere vaccine. The National Influenza Center will closely monitor which viruses are circulating outside the Netherlands and at the start of the 2025/2026 season.
The vaccine strains used in the Netherlands for the 2024/2025 season belonged to the 5a.2a.1 (subclade D.1) for A(H1N1)pdm09, 2a.3a.1 for A(H3N2), and V1A.3a.2 clade for B/Victoria. Most of the characterized influenza A(H1N1)pdm09 viruses belonged to clade 5a.2a (subclade C.1.9.3), followed by clade 5a.2a.1 (subclade D.3). All characterized influenza A(H3N2) viruses belonged to clade 2a.3a.1, with the vast majority in subclade J.2. The characterized influenza B (Victoria lineage) viruses all belonged to clade V1A.3a.2. Most were in subclade C.5.1, followed by subclade C.5.7 and then C.5.6. In laboratory tests for similarity with the vaccine viruses, most subclades of the viruses were similar to the vaccine viruses. As mentioned earlier, some of the A(H3N2) viruses had a double amino acid change in the hemagglutinin protein (HA-N158K + K189R), making them antigenic quite different from the vaccine virus.
Effectiveness of the influenza vaccine
In the 2024/2025 respiratory season, the effectiveness of the influenza vaccine against infection with the influenza virus in Europe was 46% (95% confidence interval: 40% to 52%). This final estimate, originating from the European VEBIS study, was made at the end of the winter season. In collaboration with Nivel, RIVM, like other European countries, provided data for this study. The estimate was calculated for influenza virus infections in people of all ages who visited their general practitioner with influenza-like symptoms and from whom a throat/nose specimen was collected.
Based on the number of people who visited the GP with influenza and the estimate of vaccine effectiveness, an estimate was made of the number of general practitioner visits prevented by influenza vaccination. This estimate was made for people aged 65 and older who were vaccinated within the Dutch influenza vaccination program. In the 2024/2025 season, influenza vaccination is estimated to have prevented over 3,000 general practitioner visits by people aged 65 and older.
Table 1: Overview of influenza epidemics in the past 10 respiratory seasons
| Season | Onset week | End week | Duration of epidemic |
|---|---|---|---|
| 2015/2016 | Week 1 of 2016 | Week 11 of 2016 | 11 weeks |
| 2016/2017 | Week 48 of 2016 | Week 11 of 2017 | 16 weeks |
| 2017/2018 | Week 50 of 2017 | Week 15 of 2018 | 18 weeks |
| 2018/2019 | Week 50 of 2018 | Week 11 of 2019 | 14 weeks |
| 2019/2020 | First wave: week 5 of 2020 Second wave: week 10 of 2020 | First wave: week 7 of 2020 Second wave: week 11 of 2020 | First wave: 3 weeks Second wave: 2 weeks |
| 2020/2021 | No influenza epidemic | No influenza epidemic | No influenza epidemic |
| 2021/2022 | Week 8 of 2022 | Week 20 of 2022 | 13 weeks |
| 2022/2023 | Week 50 of 2022 | Week 11 of 2023 | 14 weeks |
| 2023/2024 | Week 3 of 2024 | Week 11 of 2024 | 9 weeks |
| 2024/2025 | Week 3 of 2025 | Week 11 of 2025 | 9 weeks |
Fig 1 perc pos infl per week
Skip chart 'Figure 1. Percentage of influenza-like illness specimens positive for influenza virus from patients who visited a general practitioner, by week of specimen collection, from week 40 of 2020 through week 20 of 2025 (positive for at least 1 influenza virus). (Sources: Nivel Primary Care Database and NIC location RIVM)' and go to datatableLet op: Deze data is eigendom van de laboratoria die deelnemen aan de virologische weekstaten, vertegenwoordigd door het bestuur van de Nederlandse Werkgroep voor Klinische Virologie (NWKV(Nederlandse Werkgroep voor Klinische Virologie)). Het database beheer ligt bij het RIVM. Verder gebruik van deze data is niet toegestaan zonder toestemming. Toestemming voor gebruik van deze data kan aangevraagd worden door contact op te nemen via virweekstaten@rivm.nl.
Fig 2 IAZ en virologie influenza
Skip chart 'Figure 2. Percentage of specimens from patients with an influenza-like illness at the general practitioner, positive for influenza virus during the respiratory season (week 40 of 2024 through week 20 of 2025), by week of specimen collection and the influenza-like illness incidence per 100,000 inhabitants. (Sources: Nivel Primary Care Database and NIC location RIVM)' and go to datatableFootnote: In this figure, the ILI incidence is displayed per 100,000 inhabitants (and not per 10,000 inhabitants as in most figures), to allow for a combined display with the number of tested specimens.
Fig 3 influenza IAZ virologie NPS leeftijd
Skip chart 'Figure 3. Percentage of specimens from patients with an influenza-like illness at the general practitioner, positive for influenza virus during the respiratory season (week 40 of 2024 through week 20 of 2025), by age group. (Sources: Nivel Primary Care Database and NIC location RIVM)' and go to datatableFig 4 subtypering NIC
Skip chart 'Figure 4. Subtypes of influenza viruses sent by Dutch diagnostic laboratories to the National Influenza Center (NIC) locations Erasmus MC and RIVM during the respiratory season 2024/2025, by week of specimen collection. (Sources: NIC location Erasmus MC and NIC location RIVM)' and go to datatableFig 5 subtypering NIC leeftijd
Skip chart 'Figure 5. Subtypes of influenza viruses sent by Dutch diagnostic laboratories to National Influenza Center (NIC) locations Erasmus MC and RIVM during the respiratory season 2024/2025, shown by age group. (Sources: NIC location Erasmus MC and NIC location RIVM)' and go to datatableFig 6 infl A vir wk
Skip chart 'Figure 6. Weekly number of detections of influenza virus type A reported in the virological laboratory surveillance per week of detection, from week 40 of 2020 through week 20 of 2025. (Source: virological laboratory surveillance, RIVM)' and go to datatableNote: This data is owned by the laboratories participating in virological laboratory surveillance, represented by the board of the Dutch Working Group for Clinical Virology (NWKV). The database management is handled by RIVM. Further use of this data is not allowed without permission. Permission to use this data can be requested by contacting virweekstaten@rivm.nl.
Fig 7 infl A vir wk perc
Skip chart 'Figure 7. Percentage positive for influenza virus type A reported in the virological laboratory surveillance per week of detection, from week 40 of 2023 through week 20 of 2025. (Source: virological laboratory surveillance, RIVM)' and go to datatableNote: This data is owned by the laboratories participating in virological laboratory surveillance, represented by the board of the Dutch Working Group for Clinical Virology (NWKV). The database management is handled by RIVM. Further use of this data is not allowed without permission. Permission to use this data can be requested by contacting virweekstaten@rivm.nl.
Fig 8 infl B vir wk
Skip chart 'Figure 8. Weekly number of detections of influenza virus type B reported in the virological laboratory surveillance per week of detection, from week 40 of 2020 through week 20 of 2025. (Source: virological laboratory surveillance, RIVM)' and go to datatableNote: This data is owned by the laboratories participating in virological laboratory surveillance, represented by the board of the Dutch Working Group for Clinical Virology (NWKV). The database management is handled by RIVM. Further use of this data is not allowed without permission. Permission to use this data can be requested by contacting virweekstaten@rivm.nl.
Fig 9 infl B vir wk perc
Skip chart 'Figure 9. Percentage positive for influenza virus type B reported in the virological laboratory surveillance per week of detection, from week 40 of 2023 through week 20 of 2025. (Source: virological laboratory surveillance, RIVM)' and go to datatableNote: This data is owned by the laboratories participating in virological laboratory surveillance, represented by the board of the Dutch Working Group for Clinical Virology (NWKV). The database management is handled by RIVM. Further use of this data is not allowed without permission. Permission to use this data can be requested by contacting virweekstaten@rivm.nl.
Fig 10 clades H3N2
Skip chart 'Figure 10. Genetically characterized influenza viruses per week of specimen collection, from influenza viruses sent by Dutch diagnostic laboratories to National Influenza Center (NIC) locations Erasmus MC and RIVM, and from influenza viruses from the Nivel sentinel surveillance and Infectieradar, during the respiratory season 2024/2025. (Sources: NIC location Erasmus MC, NIC location RIVM, Nivel Primary Care Database and Infectieradar)' and go to datatableFigure 11. Estimated symptomatic influenza incidence per 10,000 inhabitants during and outside the respiratory season, as well as for the entire respiratory year, for the respiratory years 2021/2022 through 2024/2025. (Sources: Nivel Primary Care Database, NIC (National Influenza Center) location RIVM, Infectieradar).
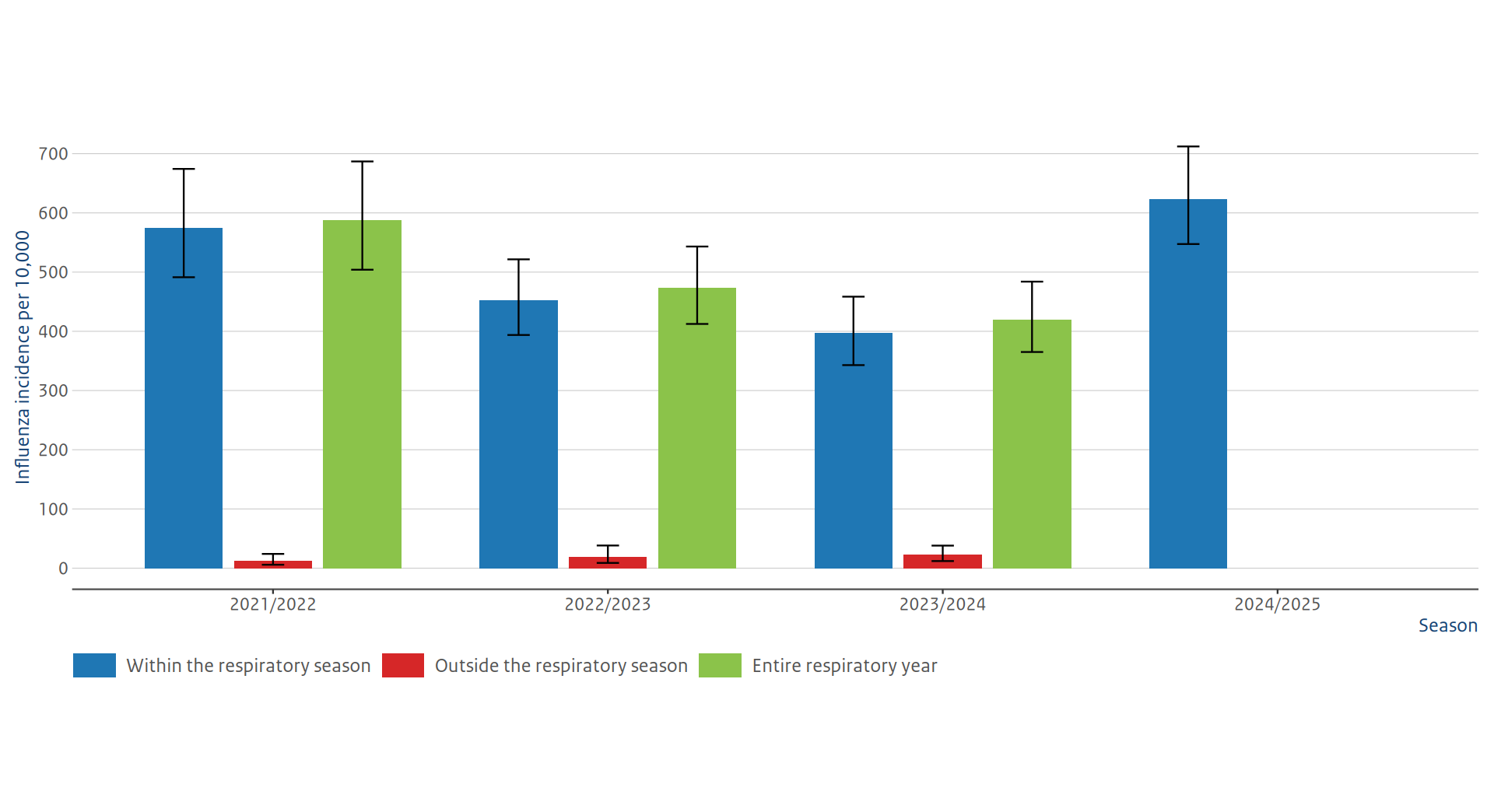
Footnote: Error bars represent 95% uncertainty intervals (UI). For the respiratory season 2024/2025 the data outside the respiratory season (from week 21 to week 39) is not yet available.
Figure 12. Estimated symptomatic influenza incidence per 10,000 inhabitants during the respiratory season by influenza virus subtype for the respiratory seasons 2021/2022 through 2024/2025. (Sources: Nivel Primary Care Database , NIC (National Influenza Center) location RIVM, Infectieradar)
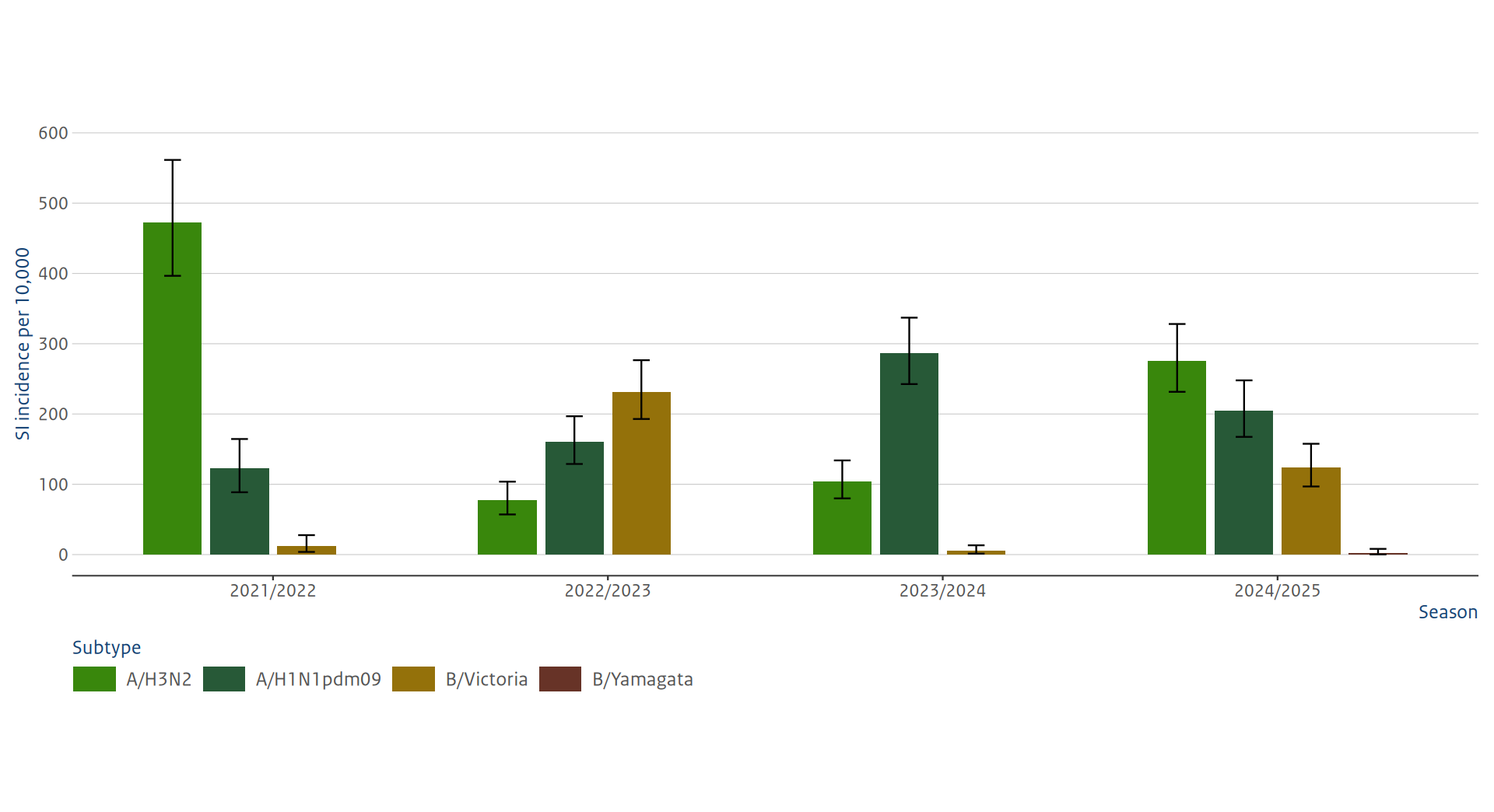
Footnote: Error bars represent 95% uncertainty intervals (UI).
Figure 13. Estimated symptomatic influenza incidence per 10,000 inhabitants during the respiratory season by influenza virus subtype for the respiratory seasons 2021/2022 through 2024/2025. (Sources: Nivel Primary Care Database , NIC (National Influenza Center) location RIVM, Infectieradar)
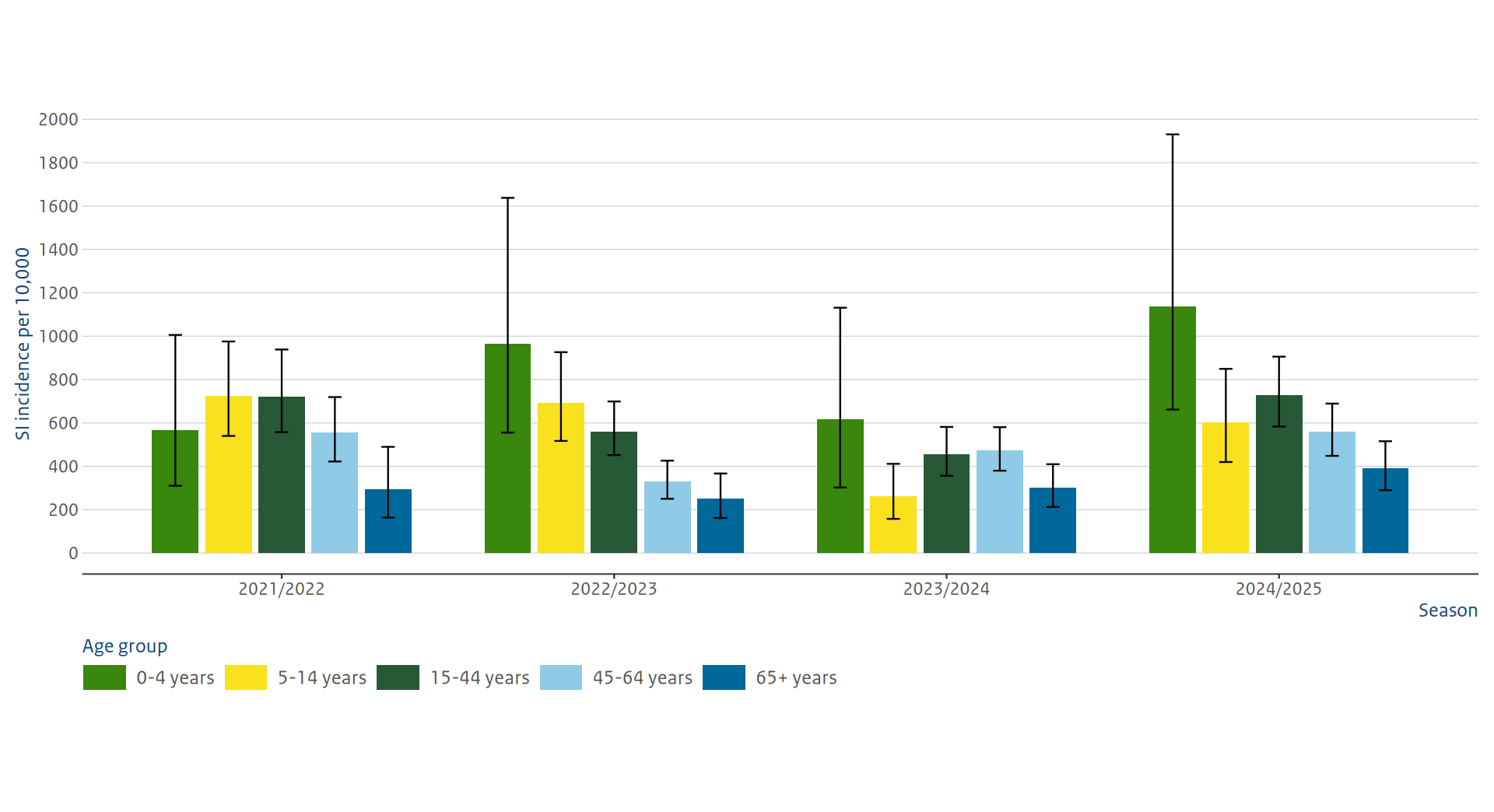
Footnote: Error bars represent 95% uncertainty intervals (UI).
Table 2. Impact estimates for influenza-like illness general practitioner consultations caused by the influenza virus for the 2024/2025 season in people aged 65 and older.
Numbers between brackets are 95% confidence intervals. (Sources: Nivel Primary Care Database, Nivel Vaccination Rate Monitor NPG (National Influenza Prevention Program), VEBIS primary care research, and NIC location RIVM).
| Used data | |
|---|---|
| Influenza vaccine coverage in people aged 65 and older1 | 64,1 (57,5 – 70,2) |
| Influenza vaccine effectiveness in people aged 65 and older2,3 | 25,2 (-3,65 – 45,4) |
| Number of GP visits for influenza in people aged 65 and older | 16.906 (12.943 – 21.461) |
| Estimated impact | |
| Number of prevented GP visits for influenza in people aged 65 and older | 3.252 (-269 – 7533) 4 |
| Number of prevented GP visits for influenza per 100.000 people aged 65 and older | 87 (-7.2 – 200) 4 |
| Number of vaccinated persons needed to avoid one influenza-associated GP visit | 708 (-3299 – 5469) 4 |
Footnote:
1. Source: Vaccination Rate Monitor National Influenza Prevention Program (NPG) 2024.
2. See the document ‘background and methods for the respiratory surveillance of 2024/2025’ for the parameters used in the calculation of the weighted effectiveness of the vaccine.
3 The vaccine effectiveness in people aged 65 and older is based on the final estimates from the European VEBIS study. These will be published at a later date.
4 The negative lower bounds of the 95% confidence interval for the results of the estimated impact show that there is uncertainty about the outcomes. This does not mean that there is a ‘negative effect’.
Fig 14. Estimates of averted GP visits for influenza for the respiratory seasons 2019/2020 through 2024/2025 in people aged 65 and older. (Sources: Nivel Primary Care Database, Nivel Vaccination Rate Monitor NPG, VEBIS primary care research, and NIC location RIVM).
Blue bars show the estimated number of observed visits. Orange bars show the estimated number of visits averted due to the influenza vaccination campaign, with 95% confidence intervals.
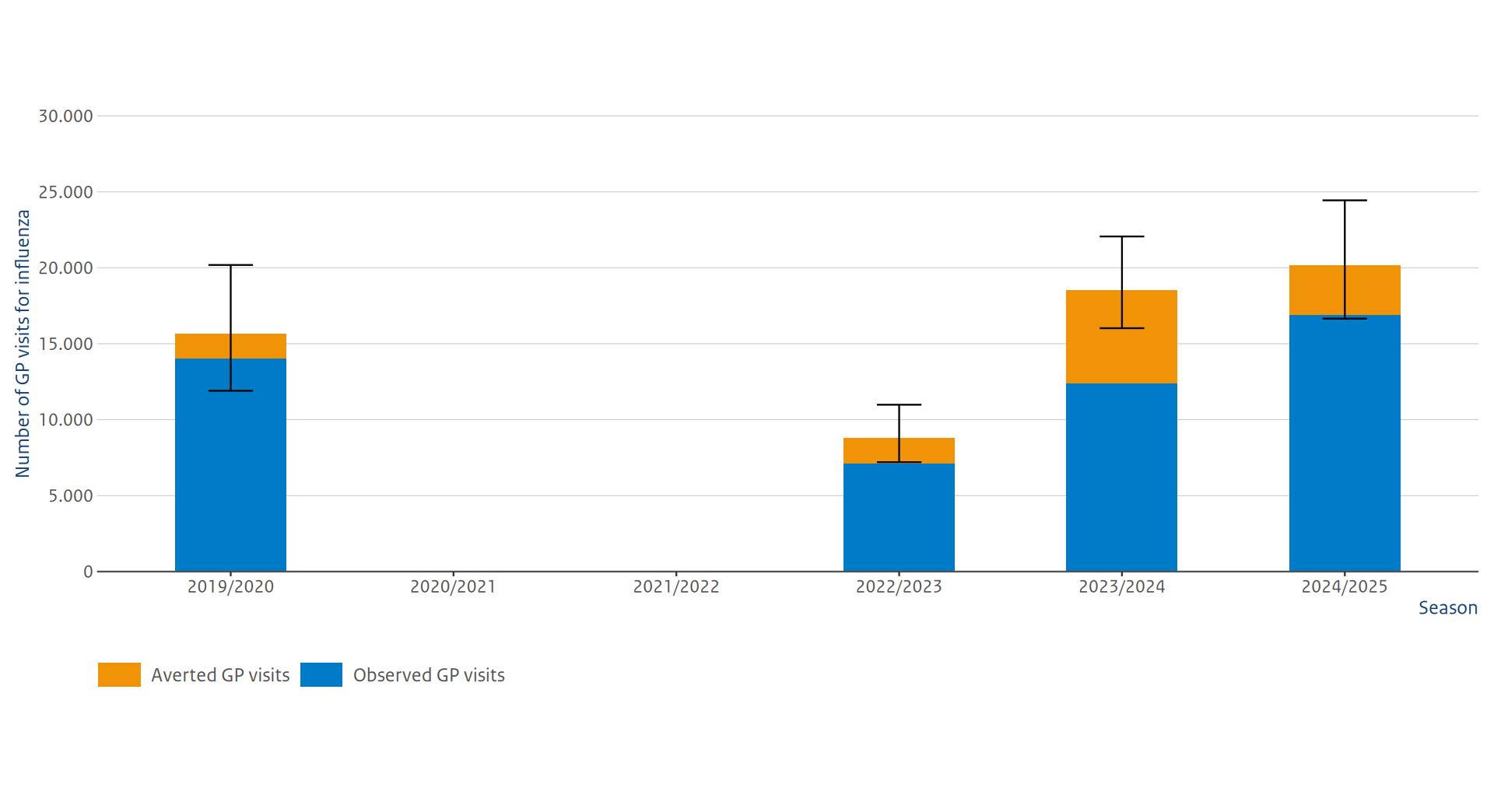
Footnote: Due to the likely changed behavior in visiting the GP during the COVID-19 pandemic, the impact for the seasons 2020/2021 and 2021/2022 was not estimated.
Contents surveillance respiratory infections
More about surveillance of respiratory infections